
Labiaplasty Minora
Labiaplasty (labioplasty) is the procedure that improves the size, shape and contour of the labia (lips of the vagina) to be aesthetically pleasing to the patient. Labiaplasty can include both or either of the labia minora and labia majora.
For the labia minora, women can be concerned about the larger size, shape, contour, asymmetry, texture and color of the inner lips of the external genitalia. For the labia majora, the most common concerns are the size, either too bulky or too thin, shape and contour, asymmetry, texture, wrinkles and color of the outer lips of the external genitalia. It follows then that labiaplasty is a general term to include multiple procedures, either medical or surgical, to address each of the concerns described above.
Dr. Michael Lau has been performing labiaplasty for over twenty-five years in Seattle, combining his training and expertise in both vaginal and cosmetic surgery. He lectures internationally on labiaplasty and has a patient base worldwide, while maintaining emphasis in serving women in the Pacific Northwest – Washington, British Columbia, Oregon, Alaska and Idaho, particularly along the Portland OR, Seattle WA, and Vancouver BC corridor. Dr. Lau performs labiaplasty using only local anesthesia (numbing medicine), and he has established a well-coordinated process that allows one-day-trip surgery not only for patients from the Seattle and Washington State area, but also those from Vancouver BC, Oregon and beyond as well.
Please view the following presentation by Dr. Lau regarding labioplasty minora, majora, and clitoral hood reduction:
Labiaplasty (Labioplasty): Labia Minora
- Most common form of labiaplasty (labioplasty). Many women have labia minora (inner lips of the vagina) that are large, hanging down beyond the labia majora, or asymmetrical. This often causes interference with clothing, intimate activities, and self-consciousness.
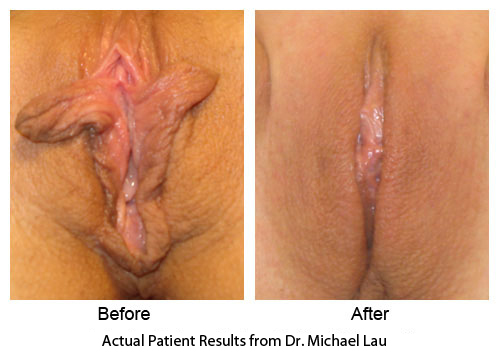
- There are different techniques for labiaplasty (labioplasty) to enhance the look of the labia minora – thinner, symmetrical, not hanging down, and less dark at the edges. Dr. Lau would recommend the best way to achieve the best cosmetic result.
Labiaplasty Image || Warning: Medical Content ||
Questions and Answers
Expert Forum by Michael P.H. Lau, MD, FACS, FACOG
What is labioplasty (labiaplasty)?
Labia, from a Latin root, a plural form of labium, are the lips of the opening of the vagina. Plasty, from a Greek root, means formed, and in a word ending it means molding, surgically forming. Labioplasty or labiaplasty means surgically molding the labia of the vagina.
Labia – what is normal?
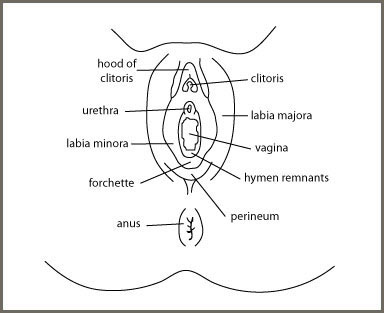
To define what is normal for the labia, one needs to understand the anatomy of the genitalia. The external anatomy of the female genitalia is comprised of the labia majora, labia minora, clitoris and the openings of the urethra and vagina.
To define what is normal for the labia, one needs to understand the anatomy of the genitalia. The external anatomy of the female genitalia is comprised of the labia majora, labia minora, clitoris and the openings of the urethra and vagina.
The labia majora are the larger outer lips, comprising skin and fatty tissue, extending from the mons pubis towards the anus. The mons pubis is the fat pad tissue right over the pubic bone transitioning to the anterior abdominal wall. The labia majora surround the labia minora and the vaginal opening. The skin over the labia majora is hair bearing.
The labia minora, comprising skin folds extending from above the clitoris, a portion called the prepuce, extend down along both sides of the opening of the vagina towards the anus to merge with the labia majora at the posterior forchette. The skin is on the outer surface of the labia minora, and the mucosa, which is the same tissue material as the vagina, is on the inner surface of the labia minora. The skin of the labia minora is not hair bearing. The nature of the inner mucosal surface of the labia minora facilitates intercourse. The labia minora are rich in nerve endings, sensitive to touch. The labia minora have a core of erectile connective tissue which swells and moistens with extracellular fluid during arousal in intimacy.
Objectively looking for what is normal for the labia, one must recognize that there is a large variation of the size, shape and color of the labia. A study published in the British Journal of Obstetrics and Gynecology in 2005 shows the following dimensions (in centimeters, 1 inch = 2.54 cm):
| Labiaplasty | Range | Average |
| Clitoral length (cm) | 0.5 – 3.5 | 1.91 |
| Clitoral glans width (cm) | 0.3 – 1.0 | 0.55 |
| Labia majora length (cm) | 7.0 – 12.0 | 9.3 |
| Labia minora length (cm) | 2.0 – 10.0 | 6.06 |
| Labia minora width (cm) | 0.7 – 5.0 | 2.18 |
82% of the genital area is darker in color than the surrounding skin. Whereas 28% of the labia minora is smooth, 68% of the labia has ridges and creases, and 4% of the labia has marked ridges and folds.
However, subjectively, the normality of the labia is a matter of perception by the woman herself, as she compares herself to what she sees of others or the “models” in the media. Often a woman feels that the labia just do not “look right” because of size, shape, color or symmetry, even though those measurements and appearances fall in the range of the objective measurement. The appearance and texture of the labia also change with increased intimate activities, child birth and aging, all contributing to the self-perception of the woman.
The most important thing to recognize is that no matter what the normal ranges are by objective measurements, the perceived abnormality of the labia by a woman is real and needs to be addressed, either by education, counseling, medical or surgical treatment.
Who should consider labiaplasty (labioplasty)?
Any woman should have the right to address her concern about how she looks and how she feels about her appearance. While people have addressed their concerns about the aesthetics of, for example, the face, the nose, the body, and so forth for years, only recently women have been more open about their concerns regarding the aesthetics of their genital areas. Besides causing aesthetic concerns, large and long labia can also cause discomfort with certain clothing and swimwear. They may also interfere with intercourse and cause hygiene issues.
Labiaplasty Majora Minora || Warning: Medical Content ||

The media has been increasingly liberal in showing images of the genital areas. Women compare themselves to those images, and even more of a concern is that their partners are comparing them to those images. Unfortunately, just as the “ideal” images of the body or faces of models in the media are unrealistic, so are the images of the models of genital areas in the media. As a result, there are increasing inquiries regarding labiaplasty (labioplasty).
Just as a person with physical or mental concerns should seek to resolve those concerns with their health care professionals, women with concerns regarding the aesthetics or function of their genitalia should address these concerns with the appropriate health care professionals. These concerns should not be taken lightly or minimized since many women bring these concerns up only after mustering much courage and deliberation. A “brush off” would be traumatizing and could make these women hesitant to express their concerns for a long time thereafter. If a health care professional does not want to or feels inadequate or uncomfortable in addressing these concerns, women should be referred to other professionals experienced in dealing with these genital aesthetic issues.
A proper evaluation of the aesthetic and functional concerns of the female genitalia should include a thorough history to explore the psychological, intimate, and physical basis of the concerns. Physical examination should be conducted with the aid of a mirror, in the presence of a female medical assistant or nurse, to understand the woman’s concern. Appropriate laboratory tests might need to be obtained.
The recommendation of labiaplasty (labioplasty) to a woman should be made only after exclusion of inappropriate psychological or intimate factors. The (labiaplasty) labioplasty should benefit the woman in improving aesthetics to address her concern and it should cause no harm.
A woman who has concerns regarding the aesthetics and function of her genitalia, after proper evaluation and counseling from a qualified healthcare professional, should be able to have those concerns addressed.
How is labiaplasty (labioplasty) done?
The plastic surgery for the labia minora is more commonly and frequently requested. This discussion of labiaplasty (labioplasty) refers specifically to the labia minora.
Labia Resection || Warning: Medical Content ||
Labiaplasty (labioplasty) can be done under local, regional, or general anesthesia. The key factor in the selection of anesthesia depends on the comfort factor of the patient and the surgeon. It is essential that both the patient and the surgeon agree on the extent and expectation of the surgery. It is proper for a surgeon to mark the areas for reduction and repair with the consent and agreement by the patient before the surgery.
The objective of the labiaplasty (labioplasty) is to enhance the aesthetics of the labia to create the desirable size, shape, color and texture of the labia, while preserving their functions, including the erectile and lubricating functions of the labia minora.
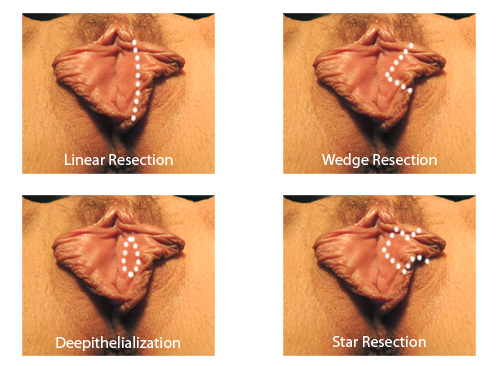
A common way to perform labiaplasty (labioplasty) is to trim off the excessive tissue of the labia by sharp dissection and then suture the edge of the incision. It is not necessary to use a laser to cut the excessive labial tissue off since that does not offer any advantage but increases the cost and complexity of the surgery. Electric cautery or cutting should be used very sparingly to prevent excessive thermal damage to the tissue and the nerve endings at the incision site. External “base ball” type of suturing can cause a railroad type of irregularity of the labia edge and should be avoided. A closure using fine sutures below the skin edges of the incision is most desirable.
Alternatively, a wedge of the labia, such as a “V” shape wedge to include the widest part of the labia or a “Z” shape wedge can be removed with sharp dissection. The incision is then closed using the same principles as discussed above. The advantage of the wedge approach is the preservation of the edge of the labia. The disadvantage of this approach is the occasional breakdown of the wedge closure, leaving a gap in the labia.
An elegant way to do labiaplasty (labioplasty) is to remove the skin and mucosa of the labia minora at the wide portion while preserving the underlying erectile tissue, nerve, blood vessels, and also the labial edge. The defect of the skin and mucosa can then be sutured together and thus reduce the size of the labia minora. The incision and repair should all be done using plastic surgery principles to minimize trauma, tissue damage, and scarring.
What are the benefits and risks of labiaplasty (labioplasty)?
Aesthetically pleasing labia after labiaplasty (labioplasty) can tremendously improve the self image and confidence of a woman. Functionally, the reduced labia allow the patient more freedom in her choices of clothing and swimwear. If patients have problems with intercourse due to large labia, the surgery should improve the problem.
Since labiaplasty (labioplasty) is superficial in location, bleeding during or after the surgery is not usually a problem that is concealed and should be able to be addressed readily. With antibiotic prophylaxis, infection is a rare problem.
Since loose tissue can shrink in different fashions with healing, there is a potential risk that the two labia may heal differently, resulting in asymmetry in size, shape and color. That can be addressed a few months later after the healing is complete by minor corrective measures.
There is also the potential risk that there is an increase or decrease in sensation of the labia after the surgery due to nerve involvement. Avoiding thermal damage of the tissue due to excessive use of laser or electric cautery and the usage of fine sutures can minimize those changes in sensitivities of the labia.
How does one find the proper surgeon to perform the labiaplasty (labioplasty)?
Both plastic surgeons and gynecologists perform labiaplasty (labioplasty). In general, rarely would plastic surgeons have training in vaginal surgery during their residency. However, plastic surgeons are skilled in the surgical techniques of resection and plastic repairs of tissues in general. With additional training in vaginal surgery, qualified plastic surgeons can perform labiaplasty (labioplasty) well.
Gynecologists are well trained in vaginal surgery and very familiar with the vaginal anatomy, pathology, and intimacy issues. They are generally qualified to do labiaplasty (labioplasty). This is especially true for urogynecologists, who are additionally trained to perform reconstructive surgery of the vagina as a subspeciality. More ideally, if gynecologists receive additional training in cosmetic and plastic surgical technique, they will have more flexibility in skills for labiaplasty (labioplasty). It is beneficial that the surgeon is skilled in all the options of labiaplasty (labioplasty) and other aesthetic surgeries of the vagina.
Can one also improve the appearance of the labia majora or hood of the clitoris?
Some women believe that their labia majora are too prominent or bulky. The labia majora can be reduced with resection of the excessive skin and underlying fatty tissue to reduce the size and improve the shape and texture of the labia majora. On the other hand, some women believe that their labia majora are too thin or have too much loose skin and wrinkles. In those cases, free fat transfer to the labia to enhance the size and shape and reduce the skin looseness can be performed with or without skin reduction.
The hood of the clitoris can be reduced if it is redundant as part of the labiaplasty (labioplasty) procedure. Occasionally, if indicated, the clitoris can be suspended to the fascia on the pubic bone to lift it up from a drooped down position.
If the mons pubis is too prominent, liposuction of the area can be performed under local anesthetic to reduce the protuberance of the mons.
What about vaginal tightening or vaginal rejuvenation?
Since labiaplasty (labioplasty) changes the appearance of the opening of the vagina, it is often requested that the vagina opening itself and maybe the vaginal canal also be tightened at the same time. This comprehensive vaginal plastic reconstruction can be done at the same surgical setting to optimize the appearance and function of the genitalia, both internally and externally.
American College of Surgeons
American Academy of Cosmetic Surgery
American College of Obstetricians & Gynecologists